
Enabling Healthy Placemaking
Recent studies have identified important challenges faced by planners who try to integrate healthy placemaking principles in their decisions. Although the barriers to building healthy places are now well-known (e.g. lack of funding; different requirements from developers; conflicting policy priorities) very few studies have given due attention to the solutions devised by planners to overcome these barriers and to create places that integrate healthy principles into the built environment. Following a call for evidence published by the RTPI in September 2019, this research explores local, national and international planning practices enabling the creation and delivery of healthy places.
You can download the report in PDF format here or read the full report below.
Please note that The RTPI runs a CPD Masterclass on ‘Planning for Public Health and Wellbeing’ each year. Please find the upcoming dates of this masterclass in the CPD Training Calendar.
If you have any question relating to CPD training, please email: training@rtpi.org.uk
Contents
- About this research
- Introduction
- Background
- Method
- Results
- Case Studies
- So what?
- Conclusion
- References
1. About this research
What is this research about?
This research explores local, national and international planning practices enabling the creation and delivery of healthy places.
Why does it matter?
Recent studies have identified important challenges faced by planners who try to integrate healthy placemaking principles in their decisions. Although the barriers to building healthy places are now well-known (e.g. lack of funding; different requirements from developers; conflicting policy priorities) very few studies have given due attention to the solutions devised by planners to overcome these barriers and to create places that integrate healthy principles (that are so integral to people’s lives) into the built environment.
Who should read this report?
Planners, Policy-makers, Public Health Professionals, Academics and anyone interested in place based approaches to health.
What kind of evidence was collected?
This is a large qualitative study based on 15 case studies and 10 interviews conducted in the UK and abroad following the publication of a call for evidence by the RTPI.
What are the key findings?
- Moving the Debate Forward. Putting principles of healthy placemaking into practice is critical – and will become even more so in a post Covid-19 context. Focusing on effective implementation rather than on normative principles is now key to addressing place-based health challenges and reducing inequalities.
- Making Collaboration Work. Greater cooperation between public health, social care and the planning profession is essential. Innovative partnerships, communication and adequate resourcing often underpin effective models of cooperation which in turn leads to successful project implementation.
- Formalising health principles in planning decisions. Our study suggests that by incorporating health needs and impact into the conceptualisation, design and planning of projects, policy makers, planners and built environment professionals are able to influence the development of sustainable communities. Our results strengthen the argument for an upstream shift to address key obstacles to healthy living via plan making.
- Equipping planners with the right skills. Leadership; Innovation; Collaboration and Negotiation were deemed essential by our respondents to overcome barriers and oppositions to healthy placemaking. Endowing planners with the right skills and giving them the opportunity to expend their knowledge and/or experience were considered critical to the implementation of health-based approaches to placemaking.
- Resourcing Planning adequately. Investing in planning is crucial to ensure the delivery of healthy, sustainable places and inclusive communities. To ‘level up’ Britain, targeted investments will be needed (especially in a post-Covid-19 economic context) across all nations and regions as well as across projects (e.g. housing, infrastructure development, high streets rejuvenation) to ensure that no places are ‘left behind’.
- Engaging the public in planning decisions. People thrive in places that fulfil their needs and which they have helped to shape. Engaging communities in planning decisions is crucial to foster social capital, a sense of community and individual well-being. Achieving these outcomes through public participation will be even more important in the design of post-Covid-19 cities to ensure the long-term success of these new, resilient and sustainable urban environments.
- Shaping the future. Unprecedented times call for unprecedented solutions. Study participants were keen to highlight the need for planners to be ‘visionaries’ in order to address the convergence of challenges around Public Health, Climate Emergency, and Economic Recovery. Harnessing the benefits of digital tools and principles of ‘green recovery’ were often cited as ‘the best ways forward’.
2. Introduction
The links between town planning and the promotion of good health are long established. As planners are well aware, town planning and public health are siblings, both emerging in the late nineteenth century to combat the unsanitary, overcrowded and inhumane conditions of industrial cities. Despite these united origins, however, the subsequent relationship between town planning and public health has proved less symbiotic.
Although health has shifted to a marginalised position within the planning agenda, where it has almost been forgotten, the short and long-term impacts of Covid-19 will almost certainly see a return of health issues back on the political agenda and, hopefully, a return of health considerations to the core of planning itself.
In recognition of the current crisis, the RTPI launched its Plan the World we Need campaign which calls on governments across the UK and Ireland to capitalise on the expertise of planners to achieve a sustainable, resilient and inclusive recovery from the COVID-19 pandemic. Our campaign aims to raise awareness of the vital role planners have in every aspect of the recovery in order to revive the economy, tackle inequality and meet net-zero targets by 2050. The COVID-19 pandemic has brought into sharp focus the strengths and weaknesses of our places and our way of life and it is now vital that we plan a greener, place-based recovery that responds not only to the lessons learned from the pandemic, but also to the challenges that we were grappling long before COVID, most notably climate change. We believe that governments must capitalise on the expertise of spatial planners to tackle place-based inequality, enable a green industrial revolution, prioritise healthy and sustainable modes of transport and coordinate the rapid deployment of zero carbon infrastructure. The campaign was launched, alongside a report, Plan The World We Need: The contribution of planning to a sustainable, resilient and inclusive recovery.
One of the most pressing task for governments across the world in the wake of the pandemic will be to draw lessons from the design of the built-environment and its impact on health. This will require decisions about what post-pandemic cities should look like in a context of climate emergency and economic recovery.
This will not be an easy task. However, when designing post-pandemic cities and their associated houses and infrastructures, policy-makers, planners and public health professionals alike will have to bear in mind the simplest yet most important lesson Covid-19 has taught us: Healthy environments make healthy people; Healthy people underpin economic vitality.
Is this something we did not know before? No. This is hardly new. For decades, planners have been working to improve health and well-being; making the case for — among other things — active travel and neighbourhood design that promote physical activity, enhance social connections and strengthen mental health. They have also long argued for compact neighbourhoods with local facilities and public transport accessibility allowing car free access to jobs and wider services. What Covid-19 has suddenly revealed is that those things do matter.
Now we have learned (the hard way) that the environment influences health, a crucial question (re)emerging is the extent to which planning can (or should) influence the environment? It is not too difficult to anticipate that in a post-pandemic context some will inevitably argue that in an effort to cut costs and speed up recovery we should do away with planning (at least, its regulatory functions). However, the imperative to keep the economy moving should not justify in the short-term, socially or environmentally damaging developments that we will live to regret.
Although started prior to the outbreak of the pandemic, our research talks to current debates in several ways:
First, our findings suggest that health policy is not only a matter for health care professionals but for the many powers and professions that affect the social, economic and environmental determinants of health. In that context planners, designers and developers all have responsibility for promoting healthy settlements.
Second, the results of our study show that the success of the planning-health dialogue is key to overcome challenges and to improve urban health outcomes. In many ways, future successes will hinge on appropriate resourcing and the active role of planners endowed with the right communication and negotiation skills.
Third, our study suggests that successful implementation of health principles in planning decisions heavily rely on public engagement and the active involvement of stakeholders in the process of decision-making. In a post-Covid-19 context – where radically new forms of neighbourhood designs and settlement patterns are likely to be desired by experts – it will be even more crucial to listen to the voices of communities who have experienced the direct impacts and consequences of one of the worst public health crises of the century.
Expending the evidence base will remain crucial to inform and guide health-focused built environment interventions – after all, as hinted by our study, there is a real need to ‘move the debate forward’ and to translate (the many) principles of healthy placemaking into practice.
We hope that the case studies and qualitative evidence gathered and presented here will help to achieve just that – by providing examples and best practices that address place based health challenges and reduce inequalities.
3. Background
Historical links between public health and urban planning have resulted in a wealth of evidence documenting the impact of the built-environment on health and well-being. Numerous studies have shown the importance of environmental and social factors in shaping both physical and mental health from a practice-based (Goldstein 1995) academic (Dannenberg et al. 2003) and policy perspective (Marmot et al. 2010; Marmot 2020).
Concepts, policies and technical strategies have been devised to bring health to the forefront of urban planning in relation to well-being, safety and environmental sustainability, with – initially – a particular focus on water and sanitation, waste cycle systems, housing and land tenure (see Freestone and Wheeler 2015).
Health based approaches have subsequently been developed in relation to transportation — emphasising the need for public transit systems that ensure sustainable forms of mobility (Pucher and Buehler 2010; Cavill et. al 2007). They also emphasise the key role of communities and social interactions on both mental and physical well-being with strong evidence demonstrating the importance of access to public amenities — including (but not limited to) medical, educational and social services (see for Halpern 1995; Wood et al. 2010).
In a similar vein, an important body of literature demonstrates the importance of securing access to safe and inclusive green spaces (Ward Thompson 2011; Swanwick et al. 2003) and access to affordable, sustainable food systems (See Soma et al.; 2011; Morgan 2013). Studies at the confluence of urban design and climate emergency have looked at – for instance – the spatial determinants of air quality (Pikora et al. 2003; Giles-Corti and Donovan 2003) and have very much drawn attention to the devastating effects of climate change on health and biodiversity (see for instance Wilson 2006; Pecl et al. 2017).
In addition to a focus on the human habitat or human experience, studies on processes and tools have also recently flourished, exploring (for example) the role of the private sector in delivering healthy places (Calcutt 2007; Williams and Dair 2006) or, by contrast, assessing the effectiveness of public frameworks and policies (see Cave 2015). In addition, the integration of health into planning policies has undergone study from an evaluation perspective – either formative or summative – with a particular focus on the value of Health Impact Assessment (Mindell et al. 2008; Bhatia and Seto 2011).
From a process-oriented perspective, a substantive amount of policy and academic work has been dedicated to public engagement and participation in planning (see Thomas 2003) — assessing, among other things, the efficacy of participatory tools and the outcomes of public engagement in decision-making (see Conrad et al. 2011).
Throughout the years, empirically based conceptual frameworks illustrating the intricate relationships between the natural/built environment and health have been developed (e.g. Whitehead and Dahlgren 1991) and influential models such as the Settlement Health Map by Barton and Grant (2006), have informed policy principles and recommendations at national and international levels (WHO and UN-Habitat 2010).
However, while planning principles for the design of healthy places are now, by and large, widely accepted (at least, at a normative level) their translation into actual intervention through design or in practice, remains often problematic.
In fact, several important studies have recently identified major obstacles hindering effective implementation of healthy placemaking principles (see Spatial Planning and Health: Getting research into Practice, PHE 2019)[1].
A 2018 report by the Design Council, for instance, explored and identified the most important barriers faced by practitioners trying to design and plan healthy places (ranked in the table below).
Table 1 – Barriers to creating healthy places
Original source: Design Council - Healthy placemaking (2018)[2]
|
|
|
|
|
Insufficient funding |
330 |
83% |
|
The requirements or expectations of developers |
327 |
82% |
|
The requirements or expectations of other professionals |
292 |
73% |
|
Other priorities that drive projects/ programmes/policies |
272 |
68% |
|
Insufficient time |
256 |
64% |
|
It’s not the norm with the external partners I work with to create healthy places |
248 |
62% |
|
The requirements or expectations of politicians |
247 |
62% |
|
National policy |
216 |
54% |
|
Local policy |
213 |
53% |
|
The requirements or expectations of senior colleagues |
171 |
43% |
|
It’s not the norm in my workplace |
143 |
36% |
|
My awareness or understanding of the actions involved in healthy placemaking |
127 |
32% |
|
My awareness or understanding of the importance of healthy placemaking |
76 |
19% |
Such studies are crucial to advance and deepen our understanding of the practical issues faced by practitioners who wish to integrate principles of healthy placemaking in their decisions. However, as the study published by the Design Council suggests, planning practitioners are incredibly ‘resourceful’ and have on occasion managed to overcome key policy, financial (and other) barriers to healthy placemaking.
Our study explores the responses and solutions of planners to challenge those barriers and find practical solutions to implement healthy placemaking principles.
4. Method
Aims and objectives
This study constitutes the first part of a larger research stream exploring local, national and international policies and best practices that facilitate healthy placemaking.
The objectives of this research stream are twofold:
1) To produce a set of practice notes describing key skills and delivery strategies necessary to implement principles of healthy placemaking.
2) To create a centralised repository of evidence where practitioners can find best practices and lessons learnt from other projects to use in their own work.
This report is an exploratory rather than confirmatory study. The overarching aim here is not to try to generalise results produced by our analyses to the entire population of planning teams in the UK, Ireland (and/or abroad), but to explore common traits among successful strategies and initiatives along with their particularities and local contexts.
Rather than focusing on a single aspect or a single feature of the built-environment (viz. housing or infrastructure development) we have adopted a wide approach to the application of healthy placemaking principles in order to identify and reflect upon the commonalities between projects of different natures and scales.
Data collection
To gain an in-depth understanding of best practices developed by planners to overcome the implementation challenges of healthy placemaking principles, we published a call for evidence in September 2019 inviting planners to reflect upon a particular project or initiative embodying successful translation of principles into practice (despite challenges). Our call for evidence was publicised on our website, promoted via our networks and remained open until December 2019.
Follow-up interviews (over the phone or in person) were subsequently organised with some of the participants – either to clarify certain points and/or to explore their answers in greater depth. Study participation was entirely voluntary.
Overall, we received 15 submissions ranging from national initiatives to ‘local’ projects. The quality of the projects submitted was checked against a list of criteria determining whether or not the entry made a meaningful contribution towards the implementation of healthy placemaking principles. We then conducted 10 follow up interviews with participants (sometimes teams of participants). Our call for evidence (Fig.1 below) comprised 11 questions asking planners to reflect upon the critical elements which facilitated the success of their projects (e.g. skills, stakeholders, tools, local context).
Data analysis
Answers to our call for evidence and interviews were analysed using traditional qualitative data analysis methods – viz. thematic analysis and qualitative content analysis (see Braun and Clarke 2012; Hsieh and Shannon 2005). Types of answers (or ‘categories of argument’) were derived from the data following an iterative process. For instance, we identified ‘collaboration’ and ‘leadership’ as key categories of argument under (Question. 3) – what kind of skills were needed to overcome barriers/obstacles or opposition? because of the recurrence of these types of answer in the responses to our call for evidence.
Figure 1 –
Call for Evidence Published 19 September 2019
ENABLING HEALTHY PLACEMAKING: Overcoming barriers and learning from best practices
|
Question 1 – |
What did you set out to achieve? Please describe in one or two paragraphs what you were trying to create, improve, change, protect (etc…)? |
|
Question 2 – |
What kind of barrier(s) did you encounter in trying to deliver your project? (You can either refer to the barriers mentioned in the table under the Background section or mention other types of barriers/obstacles). |
|
Question 3 – |
What kind of skills were needed to overcome barriers/obstacles or oppositions? (E.g. negotiation, leadership, innovation, collaboration…). |
|
Question 4 – |
Given that planning sits between many different sectors, professions and disciplines, which stakeholders were critical to making your project a success? |
|
Question 5 – |
How did you join the dots between multiple policy objectives and/or perspectives? |
|
Question 6 – |
What was the political context? Who did you have to influence and what evidence or narrative really resonated with them? |
|
Question 7 – |
Did you have to secure additional funding or resources to do things differently? If so, how? |
|
Question 8 – |
What aspect of the project are you most proud of? |
|
Question 9 – |
According to you – is the project replicable in different places or unique to this situation? |
|
Question 10 – |
What would you do differently if you were doing it again? |
|
Question 11 – |
What top tips would you give to other practitioners looking to replicate your experience/good practice? |
5. Results
1. What did you set out to achieve?
The first question in our call for evidence asked respondents to provide a short description of their project or initiative and to elaborate on what they were trying to ‘create, change or protect’.
The Background section of our ‘call’ referred to published evidence on the impact of the built-environment on health and well-being; highlighting, in particular, principles about planning for healthy neighbourhood, houses and transport as set out in previous RTPI research and policy analysis (see in particular, Promoting Healthy Cities 2014[3] and Poverty, Place and Inequality 2016[4]).
Of course, the concept of ‘healthy placemaking’ can be conceived of as ‘proteiform’ or ‘multi-dimensional’ – requiring a balance between environmental, physical and procedural elements. Throughout the years, this concept has been variously defined by academics, research/policy institutes and national/international organisations. Table 2 (below) reports some of these definitions.
By adopting a relatively wide approach to the definition of healthy placemaking we sought to elicit a variety of both substantive and procedural examples from respondents. In other words, we sought both a description of the physical aspect of their project (e.g. enhancing walkability by widening a sidewalk/pavement) and a description of a process whereby principles of healthy placemaking could be implemented (e.g. the creation of an award recognising the positive contribution of a project/scheme in improving health and well-being).
Table 2 –
|
|
|
|
|
|
|
|
|
|
|
|
|
|
“Living in vibrant, healthy and safe places and communities (…) spanning both the physical and the social aspects of place”. |
The submissions received comprised a wide variety of examples detailing the design and implementation of healthy placemaking principles – e.g. new housing developments; interventions to improve water spaces and their surroundings; organisation of workshops in County Councils in England around the theme ‘Planning for Health’.
Responses to our call for evidence also varied quite significantly in terms of the size or scale of projects, ranging from local initiatives outside the UK – e.g. Carriageway narrowing in Pune (India) – to national initiatives – e.g. the Place Standard tool in Scotland.
Table 3 below provides two examples for each type of evidence that we received, reviewed and included in our analysis. Section 6 of this report presents five case studies, which provide examples of healthy placemaking principles applied at various levels (viz. local and national). The full list of submissions selected to inform this report will be made available in our Health Evidence Repository.
Table 3 –
|
Types of Evidence/ Levels |
Examples |
|
|
ii. Active Design (England). |
|
City Council/County Council initiatives |
|
|
Local initiatives outside the UK |
i. Rejuvenation of the train station district in Grasse (France). ii. Carriageway narrowing/providing better pavement facilities for pedestrians and cyclists in Poona (India). |
We take the disparity between the scales of the different initiatives/projects as a positive rather than negative aspect of this research. Because the focus of our study is on solutions (or ‘mechanisms’) enabling successful implementation of health-based principles in planning (rather than on substantive applications of the principles) the wider the scope of the initiatives, the stronger the mechanism (or solution).
II. What kind of barrier(s) did you encounter?
Although the focus of our research is on solutions designed by planners rather than on the barriers to healthy placemaking, we did ask our participants to mention the main issues they faced when trying to implement healthy placemaking principles in their projects/initiatives.
While previous studies identified funding and issues pertaining to different expectations or requirements from developers and other professionals as important barriers (see Table 1 in Section 3 of this report) – our respondents mentioned the need to recognise key challenges associated with legislation and current policies.
Our respondents also mentioned a host of difficulties around (the lack of) expertise and (different) ‘working cultures’ across different teams, combined with the problem of accessing ‘hard to reach groups’ and/or successfully involving communities in their projects.
Table 4 –
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
III. What kind of skills were needed to overcome barriers/obstacles or oppositions?
The most important skill deemed essential by our participants to overcome barriers and obstacles to the implementation of healthy placemaking principles was (by far) the ability of planners to collaborate with other professionals (especially public health professionals but also developers).
Participants also cited ‘leadership’, ‘communication’ and the ability to ‘develop personal knowledge and new skills’ as important factors to overcome challenges.
Likewise, a number of respondents mentioned that ‘transparent decisions’ and ‘innovative strategies’ were integral to the successful delivery of their projects.
Soft skills (i.e. collaboration, leadership, ability to communicate clearly and convincingly) were also considered vital in translating principles of healthy placemaking into practice, provided the projects themselves were underpinned by adequate resourcing and aligned with broader policy objectives and priorities.
Table 5 –
|
|
|
|
|
“We worked and collaborated with transport planners, health professionals and developers (from the commercial world).” |
|
Leadership |
|
|
Communication |
“We produced a document that could easily be read by health professionals as well as planning professionals including transport planners”. |
|
|
|
|
|
|
|
|
|
IV. Which stakeholders were critical to making your project a success?
Engaging with a variety of stakeholders — ranging from public health ‘leads’ to community leaders and end users — was deemed critical to successful project delivery.
In addition, engaging with communities and developers early on in the process was considered a key component of a successful strategy.
Timing (viz. early engagement of key stakeholders) and the regularity of engagement exercises were also viewed as crucial factors towards the effective translation of healthy placemaking principles into practice.
Table 6 –
|
|
|
|
|
“Although led by the City Council [our initiative] has involved a number of stakeholders from other local authorities planning professionals, public health practitioners and [the] County Council’s Public Health Lead for healthy places and people”. “We hope we are continually promoting best practices and also have been able to keep all our stakeholders from across all sectors involved in our project. As our work programme has grown so has our network (…), including third sector and communities”. “We considered the needs of all users and functions throughout, undertaking consultation with sport and recreation clubs and neighbouring authorities, as well as the key stakeholders (the Canal and River Trust, Environment Agency and Port of London Authority). A key objective was to provide healthy, free commuting solutions, thereby inclusively planning for the disadvantaged.” |
|
Developers |
“Informal consultation was undertaken with strategic developers to evaluate the response to the process. Having a developer insight has proven to be fundamental especially when it came to the acceptability of assessments”. |
|
|
|
|
|
|
V. Other key drivers of success
Other key drivers of success mentioned by participants included adequate funding, political interest (in the project/initiative) and alignment with other policy objectives and priorities. Some respondents also emphasised the need to make decisions with a view to achieving long-term objectives and the necessity to deliver projects that maximise public benefits.
Some of these key drivers have been explored in recent studies led by the RTPI (see for instance Resourcing Public Planning 2019[9] and Investing in Delivery II 2018[10]).
The below Quotes draw on specific examples from our selected Case Studies (presented in the next section) and are taken from wider responses to our call for evidence (which will be made available in our Health Evidence Repository). These quotes demonstrate that…
Funding
“The Scottish Government and NHS Health Scotland (equivalent of Public Health England) provided a small fund for the development of the tool, which allowed myself and others to go on secondment to NHS Health Scotland. The Scottish Government and NHS Health Scotland paid for people’s time away from the office to develop the place standard tool but this was not on a full time basis – it was all done whilst we all did our other job roles as well”.
Political Interest
“There was a good deal of political interest in the work, including meetings with some Ward Councillors. Supporting the health and wellbeing of the more disadvantaged communities is a key priority for some politicians. There were also references to the ‘long memories’ of the damage caused in the 1980s by poor, less regulated development. For example, much of the river frontage was effectively privatised and parks were overshadowed by tall buildings. The unique character and quantity of the boroughs waterways, and the potential they offer, really resonated with many stakeholders.”
Alignment with other policy objectives and priorities
“The Livewell Development Accreditation Scheme can contribute to achieving a broad number of national and Essex Health and Wellbeing objectives and priorities. These align with the Chelmsford’s corporate objectives, the Joint Essex Health and Wellbeing Strategy and the National Planning Policy Framework on ensuring developments are safe, inclusive, and accessible and promote health and wellbeing. This will also help developers demonstrate their contribution to high-quality growth and delivering the EPOA’s Essex Quality Charter”.
Delivery of public benefits
“We identified the potential to deliver public benefits through overlaying mapped datasets, including surface water flooding, critical drainage, schools, stations and community facilities, access to open space and access to nature. We then validated this desk work through site visits to all open spaces, all Green Grid routes, and the Borough’s 19 water spaces. Finally, we reviewed the Green Grid and water space opportunities against the public benefits they have the potential to deliver, allowing the Council to prioritise opportunities as development comes forward.”
Long-Termism
“The challenge is promoting success to encourage further success in an area where some developers have not altered their practice and continue to masterplan around the car. The real outcome might be generational and there is a need to measure impact over a period of time”.
Networking
“Map out the network across sectors and who has common goals and work with partners in a collaborative way. Continue to evolve and develop the message to existing partners and future partners. Promote the message with key stakeholders in the same field, related fields and the future professionals likely to influence change”.
6. Case Studies
The case studies presented here focus either on processes (i.e. the development of a ‘tool’ or an ‘award’) or on specific applications (i.e. neighbourhood regeneration) of healthy placemaking principles. Examples are drawn from projects and initiatives developed at national and local levels within and outside the UK. These projects were initiated by planning professionals working:
- In the public sector (e.g. the Livewell Development Accreditation scheme developed by Chelmsford City Council in partnership with Essex County Council)
- In the private sector (e.g. the rejuvenation of the train station district in Grasse, France by the urban psychology practice ‘Hurba’)
- Collaboratively in both public and private sectors (e.g. LUC’s Connecting Communities for a Healthier Tower Hamlets project).
The specific focus of the projects vary greatly, including:
- a framework taking a holistic approach to physical and mental health (the Place Standard Tool);
- an accreditation scheme recognising the positive contribution of developers in improving health and well-being (the Livewell Development Accreditation);
- the development of a green and blue network enhancing walking and recreational activities (Connecting communities for a Healthier Tower Hamlets);
- a holistic approach to embed health in local plan development (Planning for Health in South Worcestershire); and
- the rejuvenation of a relatively rundown district using participatory practices based on business psychology principles (the rejuvenation of the train station district in Grasse).
Despite important variations in the scale and focus of these projects – shared characteristics emerged during our interviews and data analysis, suggesting that successful implementation of healthy placemaking principles (at all levels) might be helped or motivated by:
- Collaboration
- Stakeholder engagement
- Innovation
- Clear processes
- Adequate funding/resourcing
Case Study I: The Place Standard Tool
https://www.placestandard.scot/ 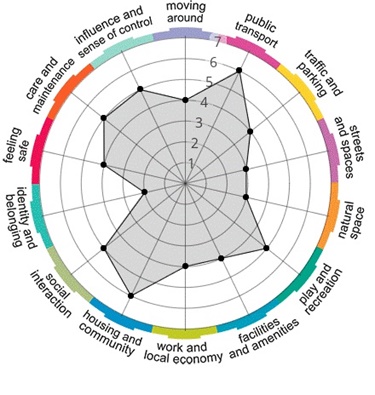 1. Description
1. Description
The purpose of the place standard tool is to support the delivery of high quality places in Scotland and to maximise the potential of the physical and social environment in supporting health, wellbeing and a high quality of life .
2. Is the project replicable in different places or unique to this situation?
The place standard tool is extremely transferrable and has already been translated into Dutch (De Leefplekmeter). Around 13 European countries are now using it including Norway, Denmark, Sweden, Lithuania and Turkey.
3. What top tips would you give to other practitioners looking to replicate your experience/good practice?
People tend to shy away from collaborative working but it really tests you as a professional, makes you think in a more strategic way and also gives you an insight into how worthwhile a few difficulties and disagreements can create.
4. What would you do differently if you were doing it again?
I would have included more practitioners from creative backgrounds, as well as local people when developing the original tool. Also I would have included way more children and young people in our discussion.
Case Study II: The Livewell Development Accreditation
https://www.essexdesignguide.co.uk/supplementary-guidance/livewell-development-accreditation/
 1. Description
1. Description
This is an accreditation scheme recognising the positive contribution that developers are playing in improving health and wellbeing through their developments.
2. Is the project replicable in different places or unique to this situation?
The scheme could be replicable for new developments elsewhere as it aims to raise health and wellbeing as a priority in new developments focusing the designing of health and wellbeing in the environment early on in the planning process.
3. What top tips would you give to other practitioners looking to replicate your experience/good practice?
-Focus on early engagement with case officers, members, health and wellbeing board and county council for Public Health, but also between planning and health practitioners.
- Ensure resources are in place for HIA assessments
4. What would you do differently if you were doing it again?
Engage further with the developer community and invite the NHS to be part of the group so that a specific section on NHS services would also be of benefit.
Case Study III: Connecting communities for a Healthier Tower Hamlets
https://landuse.co.uk/rtpi-awards/
 1. Description
1. Description
This project set out to develop an innovative water space strategy to highlight the importance of spaces for water-based transport and recreation, as well as the significant environmental and health benefits they provide.
2. Is the project replicable in different places or unique to this situation?
The project is highly replicable. The challenge of making cities for ‘permeable’ on foot and by bike is widespread and the solutions are quite similar.
3. What top tips would you give to other practitioners looking to replicate your experience/good practice?
Be ambitious while also securing some ‘easy wins’.
4. What would you do differently if you were doing it again?
If we were to carry out this work again,
we would seek further involvement of public health professionals.
Case Study IV: ‘Planning for Health in South Worcestershire’
https://www.swdevelopmentplan.org/?page_id=13484
 1. Description
1. Description
Worcestershire County Council (WCC) and the three South Worcestershire Councils have developed a holistic approach to addressing health inequalities. The project included but was not limited to a 'Planning for Health' research paper and workshops; a 'Planning for Health in South Worcestershire' SPD; secondment of a planning professional within the Public Health Directorate; implementation of Health Impact Assessments; and the integrated consideration of health in planning applications.
2. Is the project replicable in different places or unique to this situation?
The research paper and workshops were innovative approaches to addressing health issues, bringing them to the attention of District Council planners and other stakeholders through engagement and through exploring new ways of working. The creative and innovative partnership that was formed could easily be replicated by other authorities.
3. What top tips would you give to other practitioners looking to replicate your experience/good practice?
Think big and keep going. Look for alternative ways of doing things that you recognise are important issues that need addressing. So at the County Council we couldn’t produce an SPD but we were able to bring to the attention of others the importance of addressing health through planning and build relationships and pull together the key people from the districts and Public health and lead on the production of a Health SPD. Relationship building is of great importance. That is between The Public Health team and District and County Colleagues and others who will have an impact on health and wellbeing.
4. What would you do differently if you were doing it again?
Get the northern districts more involved.
Case Study V: Rejuvenation of the train station district in Grasse (France)
https://hurba.fr/en/references/
 1. Description
1. Description
This project set out to engage people in the re-development of a relatively rundown urban area (by comparison with the rest of the city) situated by the train station in Grasse (south of France). The aim was to reconnect the district area to the rest of the town centre, and to (re)foster a sense of pride and belonging among the inhabitants in the neighbourhood.
2. Is the project replicable in different places or unique to this situation?
Yes, methods and techniques used here – viz. the application of psychology principles initially designed for businesses to urban environment design – are highly transferable. These include one-to-one interviews (rather than the use of techniques exclusively involving large groups of participants); follow-up sessions and final briefings tracing decisions back to engagement exercises.
3. What top tips would you give to other practitioners looking to replicate your experience/good practice?
Listen, empathise, and get to the bottom of your interviewees’ experiences.
Safeguard transparency and accountability throughout the engagement process
4. What would you do differently if you were doing it again?
Try to get better access to ‘hard to reach’ groups.
7. So what?
7 steps to plan for healthier environments
-
Moving the Debate Forward
There is now a large body of evidence showing that planning has a critical role to play in delivering healthy places – using preventative rather than curative measures. The implementation of healthy placemaking principles is one (and arguably the most critical) preventative measure, and will become even more critical in a post Covid-19 context. Turning evidence into policy and policy into action will require re-focusing efforts to effectively apply the evidence already gathered (rather than to design new frameworks) around ‘good’ principles of healthy placemaking.
If the delivery of healthy places remains a ‘contested concept’, reaching agreement on adequate objectives that can be turned into statutory policies should be sufficient to drive future studies.
Figure 2 below provides an initial approach based on the factors that are essential to translate healthy placemaking principles into practice.
Figure 2 – Translating principles of healthy placemaking into practice
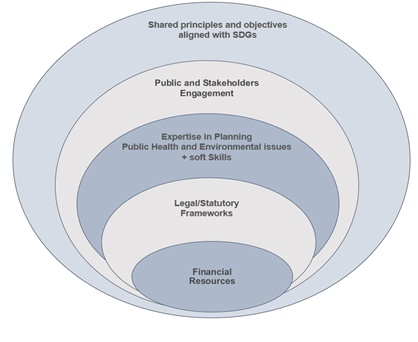
Focusing on effective implementation rather than on normative principles has now become critical to address place-based health challenges and to reduce inequalities.
-
Making Collaboration Work
Our findings very much resonate with recent conclusions from the WHO stating that “to promote better health, there is a need to break down topic silos and, specifically to promote cooperation between public health, planning and environmental sectors[12]”. The majority of planners who took part in our study emphasised the need to encourage greater levels of cooperation between public health, social care and planning professionals.
|
Innovative partnerships, communication and adequate resourcing underpin successful projects and models of cooperation between planners and public health professionals. |
Although building effective relationships across different sectors is often encouraged, collaboration remains the exception rather than the norm. Successful initiatives have been driven by the use of evaluation techniques (viz. HIAs) which strengthen inter-departmental collaboration. However, when HIAs are not an option, efforts to translate healthy placemaking principles into practice have relied heavily on shared interests and a willingness to take part in innovative forms of partnerships aligned with policy frameworks prioritising health outcomes.
-
Formalising health principles in planning decisions
An analysis of the responses to our call for evidence, including the interviews undertaken, strengthens the argument for the use of HIAs to assess the potential health effects of proposed projects and policies. By incorporating health needs and impact into the conceptualisation, design and planning phases of projects, policy makers, planners and built environment professionals are able to influence the development of sustainable and resilient communities.
This, again, echoes recent WHO recommendations stating that ‘it is important to perform health impact assessments at the planning stage to allow for the adaptation of the project at the early concept and design stages if necessary’ (Prüss-Üstün et al. 2016).
However – as often pointed out in our study – there is no formal statutory process for assessing planning projects’ impact on health, unless local policy supports the use of HIAs. Formalising the use of HIAs (via legal requirements or policy frameworks) would constitute an important step towards the implementation of healthy placemaking outcomes in planning decisions.
-
Equipping planners with the right skills
|
Our results suggest that to tackle challenges associated with the implementation of health based principles in placemaking, planners must believe in the importance of collaboration, co-production and negotiation with diverse public and private sector actors and social groups. Endowing planners with the right skills and giving them the opportunity to expend their knowledge and/or experience, were considered critical to help the implementation of health based approaches[13]. |
|
- Resourcing Planning adequately
|
The results of our analysis suggest that successful projects are underpinned by a long-term ‘vision’, fruitful collaboration, communication and adequate funding. More than ever, investing in planning will be crucial in the coming years to ensure the delivery of healthy, sustainable places and resilient communities. To ‘level up’ Britain, investments will be needed (especially in a post-Covid-19 economic context) across regions but also across projects (e.g. housing, infrastructure development, high streets rejuvenation) to ensure that regional and national disparities are addressed and no places are ‘left behind’[14]. |
- Engaging the public in planning
|
The rationale behind the support for engaging the public in planning is that ‘’people thrive in places that fulfil their needs and that they have had the ability to shape’’. For many respondents, engaging communities in planning decisions is considered crucial to foster social capital, a sense of community/belonging, and individual well-being. |
|
 Participants in our study highlighted the need for planners to be ‘visionaries’ in order to address the convergence of challenges around public health, climate emergency, and economic recovery. Harnessing the benefits of digital tools and principles of ‘green recovery’ were cited as ‘the best ways forward’.
Participants in our study highlighted the need for planners to be ‘visionaries’ in order to address the convergence of challenges around public health, climate emergency, and economic recovery. Harnessing the benefits of digital tools and principles of ‘green recovery’ were cited as ‘the best ways forward’.
How cities and regions in other countries have been addressing (and will keep addressing) health and climate-related challenges in the near future can provide useful information and benchmarks for progress towards the creation of healthier and more sustainable places in the UK.
Interviews with planners working abroad shed light on new models of healthy urban infrastructures (for instance, the concept of the 15-minute city) with the potential to reduce carbon emissions while promoting physical and mental well-being.
8. Conclusion
Summary
Recent studies have identified important barriers to the integration of healthy placemaking principles into project design and decision delivery faced by the planning profession. Using qualitative interviews and cases studies, our exploratory study gauges how planners have managed to overcome these barriers.
Our findings suggest that despite trying circumstances (e.g. lack of resources and capacity, lack of expertise and formal partnerships across teams) successful projects have been driven by planning professionals who initiated and developed collaborative, innovative and ‘integrated’ approaches to healthy placemaking.
Of course, our results are not representative of the entire planning profession in the UK (or abroad). However, they do provide an indication of the main strategies designed by planning professionals to facilitate the translation of healthy placemaking principles into practice. These strategies include:
- Effective collaboration and clear communication between planning and public health teams/professionals.
- Developing new skills and acquiring expertise in areas cutting across planning and health.
- Stakeholder engagement – especially developers and local communities.
- Clear and transparent processes.
Other key factors of success include:
- Adequate funding
- Health and well-being principles integrated into local policies (viz. local plans) and in decision-making (via HIAs).
- Political interest in the project and a wide engagement with health and placemaking at the local policy level.
- Alignment with broader (viz. national) objectives and priorities.
Responses to our call for evidence, including interviews with research participants, strongly suggest a real ‘willingness’ from planning professionals to integrate principles of healthy placemaking in their decisions. Notably, a very positive/pro-active attitude was evident in the responses received towards the creation of healthy, inclusive and sustainable places (despite important financial and policy challenges).
More often than not, efforts to collaborate with other teams and to acquire technical expertise on health-related topics in a short space of time were undertaken on an individual and voluntary basis; motivated by sincere commitments to plan for ‘the public good’. Perceptions about the threat posed by climate change were often linked (in our interviews) to considerations about the necessity to plan for healthy environments.
Overall, evidence gathered for the purpose of our study reveals a great sense of responsibility and advocacy towards planning for healthier cities, as well as a strong appetite for improved national/local guidance and stronger policies enabling the delivery of healthy places.
Next Steps and Further Avenues for Research
Going beyond qualitative interviews and case studies, opportunity exists for further research to systematically identify and quantify key factors of success that enable the creation of healthy places and, in doing so, single out potential gaps between policy aspirations and actual practices.
An important point raised by previous studies on similar topics, as well as by many of our participants, was the necessity to develop a repository of evidence where planning professionals can find out best practices from diverse projects.
As set out in the objectives of this research, the creation of a Health Evidence Repository and the publication of a set of practice notes describing key skills and delivery strategies necessary to implement healthy placemaking principles will soon follow the publication of this report.
9. References
Barton, H. and Grant, M., 2006. A health map for the local human habitat. The journal for the royal society for the promotion of health, 126(6), pp.252-253.
Bhatia, R. and Seto, E., 2011. Quantitative estimation in health impact assessment: Opportunities and challenges. Environmental Impact Assessment Review, 31(3), pp.301-309.
Bicquelet-Lock, A. and Taylor, J., 2020. The Future of the Profession – An analysis of the challenges facing the next generation of planners’ Journal of Urban Regeneration & Renewal 13 (4), pp.380-389.
Braun, V. and Clarke, V., 2012. Thematic analysis.
Callcutt, J., 2007. The Callcutt Review of housebuilding delivery. Communities and Local Government Publications.
Cave, B., 2015. Assessing the potential health effects of policies, plans, programmes and projects. The Routledge handbook of planning for health and wellbeing. Abingdon: Routledge. https://www. routledge. com/The-Routledge-Handbook-of-Planning-for-Health-and-Well-Being-Shaping-a/Barton-Thompson-Burgess-Grant/p/book/9781138023307.
Cavill, N., Kahlmeier, S., Rutter, H., Racioppi, F. and Oja, P., 2007. Economic assessment of transport infrastructure and policies. Methodological guidance on the economic appraisal of health effects related to walking and cycling.
Conrad, E., Cassar, L.F., Christie, M. and Fazey, I., 2011. Hearing but not listening? A participatory assessment of public participation in planning. Environment and Planning C: Government and Policy, 29(5), pp.761-782.
Dair, C.M. and Williams, K., 2006. Sustainable land reuse: the influence of different stakeholders in achieving sustainable brownfield developments in England. Environment and Planning A, 38(7), pp.1345-1366.
Dannenberg, A.L., Jackson, R.J., Frumkin, H., Schieber, R.A., Pratt, M., Kochtitzky, C. and Tilson, H.H., 2003. The impact of community design and land-use choices on public health: a scientific research agenda. American journal of public health, 93(9), pp.1500-1508.
Freestone, R. and Wheeler, A., 2015. Integrating health into town planning: A history. In The Routledge Handbook of Planning for Health and Well-Being (pp. 51-70). Routledge.
Giles-Corti, B. and Donovan, R.J., 2003. Relative influences of individual, social environmental, and physical environmental correlates of walking. American journal of public health, 93(9), pp.1583-1589.
Goldstein, G., 1995. Building a Healthy City: A Practitioners' Guide: a Step-by-step Approach to Implementing Healthy City Projects in Low-income Countries. WHO.
Halpern, D., 1995. Improving mental health through the environment: a case study. Mental health and the built environment: more than bricks and mortar, pp.173-233.
Hsieh, H.F. and Shannon, S.E., 2005. Three approaches to qualitative content analysis. Qualitative health research, 15(9), pp.1277-1288.
Marmot, M., Allen, J., Goldblatt, P., Boyce, T., McNeish, D., Grady, M. and Geddes, I., 2010. The Marmot review: Fair society, healthy lives. London: UCL.
Marmot, M., 2020. Health equity in England: the Marmot review 10 years on. Bmj, 368.
Mindell, J.S., Boltong, A. and Forde, I., 2008. A review of health impact assessment frameworks. Public health, 122(11), pp.1177-1187.
Morgan, K., 2013. The rise of urban food planning.
Pecl, G.T., Araújo, M.B., Bell, J.D., Blanchard, J., Bonebrake, T.C., Chen, I.C., Clark, T.D., Colwell, R.K., Danielsen, F., Evengård, B. and Falconi, L., 2017. Biodiversity redistribution under climate change: Impacts on ecosystems and human well-being. Science, 355(6332), p.eaai9214.
Pikora, T., Giles-Corti, B., Bull, F., Jamrozik, K. and Donovan, R., 2003. Developing a framework for assessment of the environmental determinants of walking and cycling. Social science & medicine, 56(8), pp.1693-1703.
Pucher, J. and Buehler, R., 2010. Walking and cycling for healthy cities. Built environment, 36(4), pp.391-414.
Skeffington Committee, 2013. People and planning: Report of the committee on public participation in planning (The Skeffington Committee report). Routledge.
Soma, T. and Wakefield, S., 2011. The emerging role of a food system planner: Integrating food considerations into planning. Journal of Agriculture, Food Systems, and Community Development, 2(1), pp.53-64.
Swanwick, C., Dunnett, N. and Woolley, H., 2003. Nature, role and value of green space in towns and cities: An overview. Built Environment (1978-), pp.94-106.
Thomas, H., 2003. Public participation in planning. In British Planning Policy (pp. 187-206). Routledge.
Ward Thompson, C. and Aspinall, P.A., 2011. Natural environments and their impact on activity, health, and quality of life. Applied Psychology: Health and Well‐Being, 3(3), pp.230-260.
Whitehead, M. and Dahlgren, G., 1991. What can be done about inequalities in health?.Lancet, 338(8774), pp.1059-1063.
Wilson, E., 2006. Adapting to climate change at the local level: the spatial planning response. Local environment, 11(6), pp.609-625.
World Health Organization and Habitat, U.N., 2010. Hidden Cities: unmasking and overcoming health inequities in urban settings. Geneva-Kobe, WHO.
Wood, L., Frank, L.D. and Giles-Corti, B., 2010. Sense of community and its relationship with walking and neighborhood design. Social science & medicine, 70(9), pp.1381-1390.
[1] PHE (2019). Spatial Planning and Health. Getting research into Practice (GRIP): study report [online]. Available at:
https://www.gov.uk/government/publications/spatial-planning-and-health-getting-research-into-practice-grip
[2] Design Council (2018). Healthy Placemaking [online] Available at: https://www.designcouncil.org.uk/resources/report/healthy-placemaking-report
[3] Planning Horizons no.3. Promoting Healthy Cities (2014). Available at:
https://www.rtpi.org.uk/media/1470/promoting-healthy-cities-full-report-2014.pdf
[4] Poverty, Place and Inequality (2016). Available at:
https://www.rtpi.org.uk/media/2212/povertyplaceinequality-policypaper2016.pdf
[5] World Health Organisation (1998). Health Promotion Glossary. Available at: http://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf?ua=1
[6] Public Health England (2017). Spatial Planning for Health: An evidence resource for planning and designing healthier places. [online] Available at: https://www.gov.uk/government/publications/spatial-planning-for-health-evidence-review
[7] Well-being of Future Generations Wales Act (2015). Available at:
https://futuregenerations.wales/a-healthier-wales/
[8] Public Health Scotland: Our areas of work (2020) Available at:
https://www.publichealthscotland.scot/our-areas-of-work/improving-our-health-and-wellbeing/scotlands-public-health-priorities/live-in-vibrant-healthy-and-safe-places-and-communities/
(Please note that definition by Public Health Scotland is currently being developed).
[9] Resourcing Public Planning (2019). Available at:
https://www.rtpi.org.uk/policy/2019/november/resourcing-public-planning/
[10] Investing in Delivery II (2018). Available at:
https://www.rtpi.org.uk/investingindelivery
[11] For a broader set of principles encouraging collaboration and community involvement and seeking to improve the impact of combined energy, resources and investment in Scotland see the Place Principle: https://www.gov.scot/publications/place-principle-introduction/
[12] Prüss-Üstün, A., Wolf, J., Corvalán, C., Bos, R. and Neira, M., 2016. Preventing disease through healthy environments: a global assessment of the burden of disease from environmental risks. World Health Organization.
[13] For further analysis on the Future of the Planning Profession please see Bicquelet and Taylor The future of the profession: An analysis of the challenges facing the next generation of planners (2020). See also the RTPI Understanding the Future Planner Pipeline research programme.
[14] See Plan The World We Need: The contribution of Planning to a sustainable, resilient and inclusive recovery (2020)
For further information about this report please contact:
Aude Bicquelet-Lock
aude.bicquelet@rtpi.org.uk


